|
|
||||||||||||||||
|
Home |
Program |
Speakers |
Meeting Registration |
Hotel Reservation |
Hotel Information |
Fellow Presentations
Voriconazole-Induced Nodular Hypertrophic OsteoarthropathyKristen Demoruelle, MD
Rheumatology Fellowship Program, University of Colorado Denver School of Medicine, Aurora, CO Objectives
Clinical PresentationA 41-year-old female with a history of allogeneic bone marrow transplant approximately 1 year prior presented with 5 months of progressively worsening diffuse joint pain and skin nodularity. Symptoms initially began in her bilateral hands, but progressed to involve her wrists, elbows, shoulders, knees, ankles and hips. The pain was severe, present at rest but worse with movement. She became wheelchair bound due to pain and joint contractures. Her past medical history is significant for chronic renal insufficiency (diagnosed 7 years prior due to lithium induced interstitial nephritis), undifferentiated connective tissue disease, aplastic anemia due to quinacrine reaction, bilateral osteoporotic femoral head fractures, invasive aspergillosis of the sinuses and lungs on chronic voriconazole for the past year. She was on mycophenolate mofetil, tacrolimus and prednisone 15mg/day at the time of evaluation. 



Figure 1 (above). Radiographs of the left hand, left elbow, left hip and left shoulder demonstrating diffuse nodular periostitis (click photos to zoom)
On joint examination, she had warmth and tenderness of bilateral hands, wrists, elbows, ankles and feet. She had limited range of motion and flexion contractures of all joints including curl of fingers 10°, wrists 5°, right elbow 20°, left elbow 0°, knees and hips 20° and ankles 10°. She had hard nodules over her fingers, elbows and ankles. She had no clubbing. Laboratory studies revealed markedly elevated alkaline phosphatase(ALP) 475 U/L (39-117), bone specific alkaline phosphatase(BSAP), and urine N-telopeptide 326 nM BCE/mM (26-124). X-rays revealed nodular periostitis most significantly involving proximal long bones. This atypical presentation of hypertrophic osteoarthropathy (HO) with lack of clubbing, very high BSAP and proximal distribution of nodular periostitis, led to a diagnosis of voriconazole-induced nodular HO. Her pain completely resolved within one week of stopping voriconazole, but her radiographic abnormalities persisted.
DiscussionHypertrophic osteoarthropathy (HO) is a syndrome of excessive skin and bone proliferation. It classically presents with digital clubbing, symmetric painful distal joints and non-inflammatory joint effusions. X-rays typically demonstrate linear periostitis of the distal diaphysis of long bones. 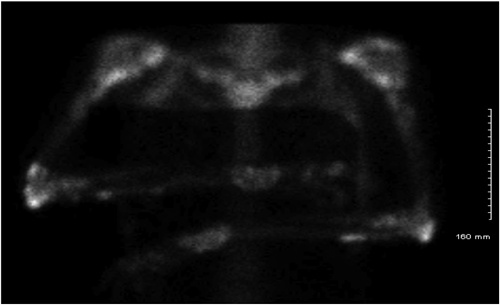

Figure 2 (above). Technetium 99m bone scan showing increased radionuclide uptake at multiple sites (click photos to zoom).
Primary HO is a hereditary disorder involving a mutation of the enzyme 15-hydroxyprostaglandin dehydrogenase which is responsible for degrading prostaglandin. These patients have excessive levels of prostaglandin E2 (PGE2)1. PGE2 causes peripheral vasodilation (clubbing) and osteoblast stimulation(periostitis). Secondary HO is associated with an underlying medical disorder, often lung cancer, right-to-left cardiac shunt or cystic fibrosis. Elevations of various cytokines including vascular endothelial growth factor (VEGF), platelet derived growth factor (PDGF), and PGE2 have been implicated in the pathogenesis 2,3. PDGF and VEGF induce new bone formation and vascular hyperplasia. A limited number of case reports of voriconazole-induced nodular periostitis have been described in the literature4,5,6. All reported cases included lung transplant patients on voriconazole from 6-24 months. Similarly, these cases also presented with severe joint pain, limited ROM, absence of clubbing, markedly elevated ALP and BSAP and radiographic evidence of symmetric nodular periostitis in proximal long bones. Rapid resolution of symptoms with discontinuation of voriconazole was also similar among all cases. The mechanism of action of voriconazole induced periostitis may be related to elevated cytokines similar to secondary HO including VEGF, PDGF and PGE24. It is interesting this patient had a markedly elevated VEGF level but a normal level of PGE2. Newer theories include fluoride toxicity, as seen in periostitis deformans, due to voriconazole’s chemical structure which includes three fluoride moieties5,6. This case demonstrates a unique presentation of HO induced by voriconazole. Voriconazole is the initial treatment of choice for invasive aspergillosis and awareness of this severely painful and disabling side effect is important for clinicians who treat immunocompromised patients. References
| ||||||||||||||||
|
Administrative Office: Contact: Home | Program |
Speakers | Meeting
Registration | Hotel Reservation | Hotel
Information | Fellow Presentations |
